Here is my module #2 in my spina bifida education month.Spina Bifida is the birth defect that sets off a chain of other problems that make up the entire package. Spina bifida comes as a package deal. There are effects on the whole body. The spinal cord, the brain, the bladder and bowels, muscles and bones, and other medical problems.
I will talk about the bladder and bowel issues in another post; these issues develop because of nerve damage to the areas that go to the bladder and bowel. But the other most common ‘tag-alongs’ to Spina Bifida are problems in the brain, (chiari II malformation, hydrocephalus), as well as problems with the bones (feet, hips, spine).
So you aren’t looking at just the back-thing, there is a whole bunch of things that come with it. Luckily someone who has Spina bifida does not necessarily have all of those problems, and hopefully if they do, they don't all cause problems at once.
Nickolas has Chiari II malformation and hydrocephalus. Luckily his feet and hips are fine and he doesn’t have any orthopaedic problems. But the effects of Spina bifida can result in problems with joints, misshapen bones, hip problems and curving of the spine. If you are missing one of two (or more) of the building blocks the tower doesn’t necessarily stay straight.
In my last education post I discussed a bit about Spina bifida, but what about the other stuff?!
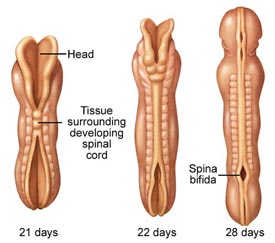
The spinal cord is only so long and when it comes out of the back, in the lesion, it pulls on the cord, which is attached to the brain, and the brain, specifically the cerebellum, is pulled down as well. This is called the Chiari II Malformation, it is the banana sign that is often noted on ultrasounds, along with the lemon sign (I’ve mentioned it before, but those radiologists must have had the munchies or something when they came up with the names of things.)
Considering the importance of the cerebellum (it is what makes you breathe among other things) – this freaks me out. But Chiari may be present and have no symptoms. The most common are problems are gagging easily as well as breathing problems or loss of upper body strength. There is a surgery (called a decompression) that can help if problems develop.
There are other types of Chiari malformation (type I – IV, but it is type II that is associated with Spina bifida). Interestingly Chiari malformation has been on recent TV shows this past season, specifically House and CSI.
Hydrocephalus occurs when the cerebral spinal fluid (CSF) cannot properly be absorbed by the body and starts to build up in the ventricles (pockets) of the brain, which makes them bigger. It is associated with Chiari because the brain tissue can block the normal flow of the spinal fluid. Spinal fluid surrounds the spinal cord and goes from the nerves and spinal cord to the brain and is then absorbed. But when the absorption of fluid is blocked it starts to enlarge the ventricles and put pressure on the brain. In babies the head is soft and so the head gets larger – that was how Nickolas’ hydrocephalus was discovered; his head grew 2.4 cm in 5 days! Once the skull fuses, kids and adults with hydrocephalus would get headaches (no kidding!) among a range of other symptoms. Even to the point of 'sunsetting' of the eyes because the pressure of the brain cause the eyes to look downwards.
Hydrocephalus is very common with Spina bifida. The most common ranges I've seen in research has been from 85-95% of people with Spina bifida also have hydrocephalus. It can develop inutero, or after the surgery, or really any time (but most common in the first year). In Nickolas’ case the hydrocephalus developed after his back was closed – before that - the system, think of it like a garden hose, had sprung a leak, so the pressure did not build up when it was blocked because there was a hole in the hose (the lesion). When the hole was closed (back closure surgery) the hose starts to build up pressure.
How painful does this picture look - can you imagine the pressure that would put on your head?! Where would the brain go when the insides start blowing up like that. It finds a way. But we really don't want to let it go that far. SHUNT HAPPENS.
But there is a treatment (not the perfect solution, but has worked well so far ***knock on wood**). To treat hydrocephalus a shunt is inserted in the brain (into the ventricles) that helps to take the extra fluid and ‘shunt’ or move it down into the abdomen where it can be absorbed by the body. Simple enough right? Yes as long as the shunt doesn’t get blocked or infected or just stops worked and so then needs a ‘revision’. Nick’s shunt is located above his right temple, in his hairline. (He was part of a study which helped to pick the right placement for the shunt by ultrasound). He also has a scar next to his belly button which is where the shunt ends.
Nickolas luckily did not have any problems with his feet or club feet, so I’m not going to go into this, other than mention that clubbed feet and other orthopaedic [bone] problems is very common with babies, children and adults with Spina bifida.
Hope you’ve learned something in this Spina bifida learning module. A lot of this information came from the MOMS study website that is being done in the States – investigating how intrauterine surgery affects the rates of needing a shunt or developing hydrocephalus. This information can be found
here.

























{kind=link}
{kind=link}